
Emergency Rectal Hydration in Remote Environments
In the 1990’s Camelbak’s moto was “Hydrate or Die!” and they weren’t wrong. Proper hydration is fundamental to life and an important component in both the emergency and long term treatment of the casualty but getting some casualties to drink water is either not possible or, in some casualties, not advised. Frustratingly, these are often the casualties who need hydrating the most:
Unconscious
How do we hydrate, or rehydrate, an unconscious casualty?
Nausea
Casualties suffering from Heat Illness are in desperate need of rehydration but the symptomatic nausea of their condition may mean that they cannot keep fluids down.
Shock
A casualty in hypovolaemic shock needs fluids but should not be given anything to drink as activation of the digestive system will redistribute blood towards it, away from the vital organs.
The experienced clinician will be able to provide fluids either intravenously (IV) or increasingly intraosseosly (IO) and on some ‘medic’ courses you may be shown IV or IO infusion techniques. This is an advanced skill and typically shown to candidates to enable them to support a more experienced medic in the familiarisation and setting up of equipment rather than promoting individuals to administer fluids by these routes under their own initiative.
But what about the medic untrained in these techniques or without the equipment and fluids?
Proctoclysis – rectal rehydration
Rectal infusion (proctoclysis) was effectively employed as an emergency treatment during the First World War for combat casualties and routinely used for infusion in clinical settings before the development of IV techniques and equipment rendered the technique redundant.(1) Early studies demonstrated the colon can retain up to 500mls of fluids per hour (2). In 2005 a now often cited article described an occasion where improvised proctoclysis in a remote setting was effectively used to treat and initially stabilise a casualty in a remote setting, re-igniting discussion on this technique as an emergency treatment in a remote environment. (3)
Rectal Rehydration can provide a simple, safe and effective means to rehydrate a casualty who is unconscious or nauseous and with less risk of adversely affecting their haemodynamic balance. The technique requires neither sterile fluids, special equipment or specific training (4-7)
Proctoclysis may be of benefit for those who work in developing countries or rural areas, where there can be little access to hospital care or where sterile cannula, fluids and giving sets are expensive. It could also be useful in mass casualty situations where clinical teams must administer fluid resuscitation despite having insufficient intravenous equipment or nursing staff. (8) The primary aim of proctoclysis in such emergency situations is to provide initial fluid resuscitation in advance of rapid evacuation for further care in a dedicated medical facility. (3)
Equipment
The 2005 article explains the improved use of a Foley catheter for rectal infusion. This is specialist piece of equipment and unlikely to be found in any First Aid kit, what the remote medic might have at their disposal is a Camelbak style hydration system and tape. A couple of other simple, small and cheap items make the following process a little easier and more effective.
Camelbak style hydration system. Theirs, not yours.
Water-based lubricant
1 Ltr clean water
Tape
Oral Rehydration Solution
Sheets / blankets
Preparation:

Explain the procedure to the patient and gain informed consent (if possible).
Maintain dignity and privacy by screening the area or casualty but request a witness if dealing with a minor, or there is a cultural or gender difference.
Filter and boil water if taken from a natural source.
Warm water to as near to body temperature as possible or to 40oc for the hypothermic or hypovolaemic casualty – not so hot that it can’t be tolerated by dipping your elbow in it.
Dissolve sufficient rehydrating solution into warmed water.
The rectal-sigmoid colon junction occurs 10-15cm from the anus. Mark the drinking tube 7.5-10cm from the end with tape (9). This will show maximum insertion depth and also reveal if the tube has moved from its position.
Fill the Reservoir with the rehydration solution.
Invert the reservoir, open the mouth piece of the drinking tube and squeeze any air out from the reservoir or tube. Close the tube once the air has been purged.
Insulate the reservoir with clothing - a litre of water at 37°C cools to about 32°C within 15 min when left at room temperature.
Fluid choice
In rectal fluid infusion, sterility is not as fundamentally important as it would be in IV or IO infusion but it is still best practice to boil or sterilise the water, especially in areas of poor sanitation or during an outbreak of infectious disease.
Water will be absorbed into the mucous membrane of the colon but not in the same way as a porous material would (such as sponge) which works on capillary action. Water is absorbed and transported across the mucous membrane using sodium ions. Without the sodium, much of the water will be flushed out creating an enema.
In some parasitic and bacterial outbreaks, ion transport is impaired meaning water from the colon is not reabsorbed, hence the diarrhoea. The one ion-transporter which is unimpaired is the glucose-sodium cotransporter which uses glucose to aid sodium (and therefore water) reabsorption. As such, including glucose into the solution will aid fluid infusion.
While clean water would do, sterile water would be better and Oral Rehydration Solution containing both sodium and glucose, such as Dioralyte®, for example, would be ideal
Procedure
Ask or assist the patient to lower clothing below the waist.
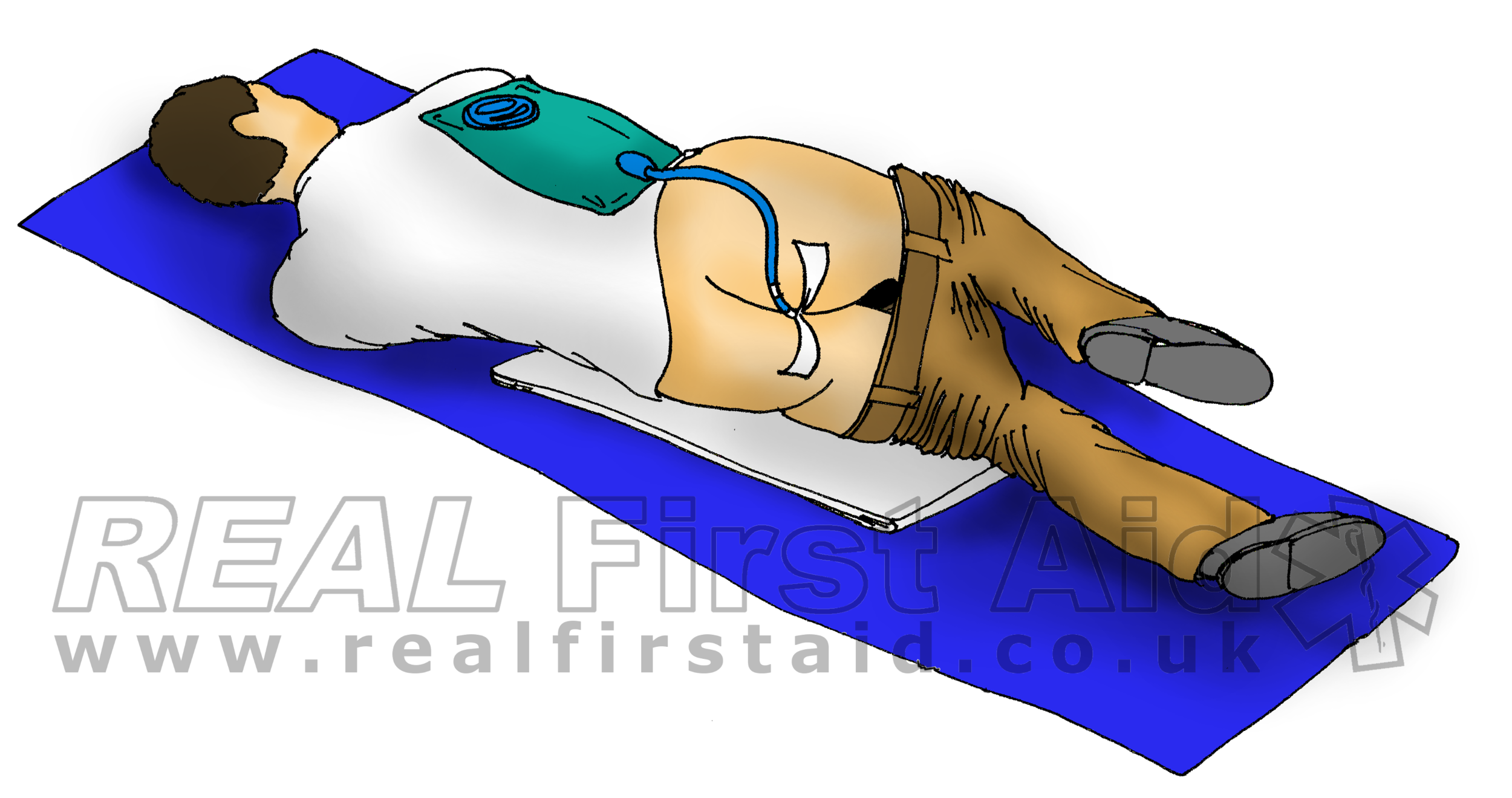
The casualty is positioned in the Safe airway Position on their left side. The sigmoid colon bends to the casualty’s left. Positioning on this side encourages fluid drainage into the colon.
Wash hands with soap and water or use alcohol gel. Dry hands thoroughly.
Wear protective gloves (if available).
If water-based lubricant is available (for use with laryngeal airways), lubricate the tube sparingly. In extremis, lubricate the tube with antiseptic cream. Do not be tempted to use sun cream, moisturiser or anything fragranced. Over-lubricating the tube will also increase the likelihood of the tube coming out or going in too far.
Remove the entire mouth piece from the drinking tube and cover the open end with your gloved finger to prevent fluid loss.
Insert the tube 7.5-10cm into the anus, proportionate to the casualty’s height. The main risk is perforating the rectum wall (10).
Take a loop of tape around the hose. Close to the anus, and anchor each end to each buttock. This will a) bring the buttocks together to reduce fluid loss and b) prevent the tube from moving.
Lay the reservoir on top of the casualty’s body.
Package and insulate the reservoir with the casualty to limit heat loss from the reservoir.
The system is gravity-fed, allowing the rectum to absorb only what is needed. Do not be tempted to force fluid into the rectum. They won’t like it. Neither will you.
Monitoring
Recheck the fluid bag. When topping up, record volumes given and at what time. Absorption rates and time frames will be required at handover.
Monitor vital signs. Significant findings are breathing rate returning to a normal range and a detectable radial pulse.
Co-ordinate ongoing transport as soon as possible.
Liaise with the receiving hospital about the need for intravenous access, fluids or blood.
Potential problems include leakage, bowl movements and flatulence.
References
Nanson J. (2000) “Methods of fluid administration for resuscitation and hydration in difficult circumstances: part 2, alternative routes.” Tropical Doctor. 30(3): 172-175
Robertson OH, Bock AV (1919) “Blood volume in wounded soldiers: II. The use of forced fluids by the alimentary tract in the restoration of blood volume after hemorrhage”. Journal of Experimental Medicine. 29, 2, 155-171
Grocott MP, McCorkell S, Cox ML (2005) “Resuscitation from hemorrhagic shock using rectally administered fluids in a wilderness environment.” Wilderness and Environmental Medicine. 16, 4, 209-211.
Girisgin AS, Acar F, Cander B et al (2006) “Fluid replacement via the rectum for treatment of hypovolaemic shock in an animal model.” Emergency Medicine Journal. 23, 11, 862-864.
Bruera E, Schoellar T, Pruvost M. (1994) “Proctoclysis for hydration of terminally ill cancer patients.” The Lancet. 344:1699
Tremayne V. (2009) “Proctoclysis: emergency rectal fluid infusion”. Nursing Standard. 24(3):46-8
Steiner N, Bruera E (1998) “Methods of hydration in palliative care patients.” Journal of Palliative Care. 14, 2, 6-13.
Girisgin AS, Acar F, Cander B, Gul M, Kocak S, Bodur S. (2006) “Fluid replacement via the rectum for treatment of hypovolaemic shock in an animal model“. Emergency Medicine Journal. 23:862–864.
Wang H, Higgins TJ, Robinson RD. (2019) “Proctoclysis”. Chapter 19 in Reichman's Emergency Medicine Procedures. 3rd Ed. Reichman EF. McGraw Hill.
Iserson KV (2012) Improvised Medicine: Providing Care in extreme Environments. McGraw Hill. New York. 141-142